Biological Effects of Electromagnetic Radiation
ARTHUR W. GUY, FELLOW, IEEE
I. MEDICAL APPLICATIONS AT SUBMICROWAVE FREQUENCIES
19th Century
It is interesting to note that it has only been since 1979 that heating tissue for control of cancer has become widely used in oncology clinics, hospitals, and cancer research centers. Yet, the first use of electric-field heating for control of cancer occurred only four decades after Volta, in 1800, described the electric pile [174]. This application' of electric current for destroying cancer through heat was demonstrated by Recamier and Pravaz in the destruction of uterine cancer [107]. In fact, the practice became so widespread in the following few years that Pichard [139], in 1846, called attention to its over use. There was considerable competition in the mid19th century between these early researchers for recognition of being first to apply electricity for heating tissue.
Becquerel [14] credited Fabre-Paloprat [44] for first burning tissue with an electrified platinum needle in 1830, but Petrequin claimed to be the first to come up with the idea based on his reading a book on electropuncture published in 1823 [107].
The early application of electricity to medicine named Galvanocautery, after Luigi Galvani, in 18th century obstetrician and surgeon in Bologna"for his work on chemical effects of electric current, involved dc currents applied directly to the tissue through needle, wire, or knife-type electrodes. The technique was reported to destroy tumors, aneuryisms, and fungoid growths, as well as to close fistulas and to stop bleeding. It was actually the caustic effect of the electricity in coagulating blood, rather than to heating effect, to which these early physicians attributed the beneficial effects. Oscillatory sources soon became available through the work of Helmholtz, Kelvin, and Hertz. Joubert, in the year 1889, demonstrated that when the frequency of current applied to frog muscle was raised to a certain level, it would not cause the muscle to contract.
In the following year, d'Arsonval (Fig. 1),

a physicianphysiologist with a strong professional interest in electrical engineering (one of the, world's early bioengineers), began research on measuring the electrophysiological activity in muscles and nerves, as well as the effect of low-frequency currents on muscles. In measuring the intensity of muscle excitation as a function of frequency, he noticed that the excitation decreased until it was barely noticeable at 10 kHz, the maximum attainable frequency of his source. He was able to apply the high-frequency current to himself at a high level without sensing anything but a warmth.
D'Arsonval was looking for physiologic rather than thermal effects. Though the immediate sensation of the currents passing through his hands from large electrodes were nil, he found that after a period of time the skin was flushed with increased sweating. He attributed this to vasodilation rather than a heating reaction and wrote that the high-frequency currents would be a great service to therapeutics, thinking in terms of direct effects on blood pressure and kidney output, rather than the indirect effect of heat. Continuing his work with equipment capable of generating frequencies of several hundred Hertz, d'Arsonval reported in 1891 that he could get no physiological effect at all at frequencies above 10 kHz, and, in 1892, a paper he sent to the French

Academie de Medecine was regarded so skeptically that it was nearly rejected (Fig. 2). To prove the sound basis of his conclusions, d'Arsonval demonstrated the use of his apparatus (Fig. 3) in courses at the College de France, Society of Electricians, to students, and finally to an Academy of Sciences Commission.

The recorder of the commission wrote in July 1893: M. d'Arsonval has produced evidence before M. Marey and myself of the principle results recorded in the previous note. We were particularly struck by an experiment in which 6 lamps (150 volts X0.8 ampere) were made luminous by a circuit formed by our arms, the circuit being derived from the ends of a solenoid induced by oscillating discharges. We have not experienced the best sensation by the passage of the current flow to which we were submitted, while one could not doubt the enormous amount of energy which passed our bodies (900 volts X 0.8 ampere) equaling 720 watts or about 1 horsepower. It manifested itself either by the luminousness of the lamps or by lively and numerous sparks which were produced when the circuit was broken. The same amount of energy would have sufficed to destroy us like lightening, but under the above given conditions it produced no appreciable sensation. [Special d'Arsonval Jubilee issue of Archives of Physical Therapy, X-Ray, Radium, 1932.]

After using a better oscillator that he devised which came to be widely used for medical purposes (Fig. 4), d'Arsonval, in 1893, reported there being no action on sensibility or contractibility; no analgesia at the electrode contact point; no vascular dilation and reduced blood pressure; and no increased metabolic rate without a rise of the central temperature but with greater heat at the periphery.
Up until 1893, all medical applications of high-frequency currents were made by direct electrical contact with the tissues or conduction. At that time, d'Arsonval introduced what he called autoconduction, which was really induction. At first, he experimentally placed animals (and then humans) in induction coils. The human-size solenoidal coils were huge with big gaps between the turns (Figs. 5 and 6).
Autocondensation, the forerunner of diathermy, remained popular for many years, especially with many optimistic reports being made. These historic coil applicators are on display at the Wellcome Museum in London, and the Bakken Museum of Electricity in Life in Minneapolis, MN.
D'Arsonval was able to obtain considerable help from Oudin as a collaborator in the clinical applications of high-frequency currents in which a resonant coupled circuit (Fig. 7) worked especially well; in addition to its medical uses, it played an important part in the development of radio telegraphy in France [169].
During the period 1894-1895, d'Arsonval clinically treated seventy-five patients suffering various ailments with his machine. Each was exposed for 15-20 min daily in the induction coil for a total of 2500 treatments. He found that most types of hysteria and certain forms of local neuralgia received no benefit, while on the other hand there was marked improvement in the health of patients suffering from arthritic, rheumatic, and gouty conditions. In extending the methodology to hospital trials, d'Arsonval introduced capacitive coupling of the electric fields to the patients in what was called a condensor couch. The patient reclined on a large, shaped, metal plate with insulating dielectric cushions (Fig. 8). The patient's body formed one electrode of the capacitor and the couch the other. Other patients were treated by having conduction currents pass from the feet in a footbath to the hands in contact with electrodes. A current of 350-450 mA was used for daily treatments of 6 min. At that same time, Tesla was also conducting similar experiments in America, showing that 20-kHz oscillations not perceived by the human body could light up nearby glow tubes or heat metal objects.
Susskind [169] has made note of the fact that unlike the pioneers of radioactivity and ionizing radiation whose health was effected and lives shortened by their experiments, d'Arsonval (1851-1940), Tesla (1856-1943), and other radiofrequency pioneers, e.g., Eli Thomson (1853-1937), all lived well into their 80's. Tesla conducted a number of experiments on himself and noted that the physiological effects, depending on voltage, current, and waveshape, were not only heated tissue, but were also changes in perspiration, blood circulation, and fatigue bordering on somnolescence. Tesla lectured on both sides of the Atlantic, and electrotherapy became very popular with an entire professional society: the American Electro-therapy Association devoted itself to the subject. Tesla reported his work at a meeting of that Society in 1898. Eli Thomson, who associated with Tesla on his lecture tours, was credited with publishing a circuit for providing high frequency fields for therapy in Turner's Manual of Practical Medical Electricity in 1897.
With widespread use of the d'Arsonval current by physicians in France, many extravagant claims were made of its effectiveness; however, others failed to replicate them. Typical of today, newspapers in 1899 published a sensational report that Tesla had cured pulmonary tuberculosis with high-frequency current, following a suggestion by Tesla of that possibility, based on his findings that high frequency current passing directly through bacilli killed them. Freund [50] wrote, in 1904, that clinical trials fell far short of what had been expected, "Consequently in some quarters the whole method received unqualified condemnation."
According to Cumberbatch [28], the actual heating mechanism of the high-frequency currents was first elucidated by Von Zeynech in 1899, who believed that the heat was produced by the passage of current through tissues just as it would when passed through other resistance.
20th Century
In September 1907, at a medical meeting in Dresden, Franz Nagelschmidt [126] demonstrated "Durchwarmung” with high-frequency currents, and in 1908, in Budapest, he demonstrated a more powerful and effective machine which left no doubt about the deep-heating effect of highfrequency currents. He coined the word diathermy to describe the procedure, and published the first textbook on the subject in 1913. By 1910, diathermy machines were beginning to make their appearance in supply houses.
Diathermy was soon used for many conditions including arthritis, poliomyelitis, pelvic diseases, pneumonia, and received its greatest publicity in 1929, when the King of England's health was improved by its use [107]. Prior to this time, a physical therapy clinic would have been a noisy place with minor thunderclaps from spinning static wheels and the humming and singing of spark gaps (Fig. 7).
Though Lee de Forest constructed the first radio tube high-frequency medical apparatus in 1907- the "Cold" cautery for electrosurgery-American surgeons refused to use it for many years. It was being used effectively by physicians in Paris and Vienna. The frequency of the current used in long-wave diathermy up to 1929 was approximately 1 MHz. Though these early generators were spark-gap oscillators, they were in vogue from 1908 to 1940. In 1928, shortwave diathermy was introduced when Esau, a physicist in Jena, constructed for Schliephake at Giessen a machine which was capable of delivering 400 W at 100 MHz [107]. Schliephake [152], [153] was the first to use the higher frequency shortwave diathermy clinically, by first using it on himself to cure a furuncle on the nose. He believed that shortwave diathermy had a selective or specific , bactericidal effect. He did much basic work on the heating of animal tissues. Schereschewsky [150] placed small animals in a condensor field of a 2-36-m apparatus capable of delivering 7.5 W. With his ability to kill flies with the apparatus, the press responded by calling it the new death ray. In 1935, manufacturers large and small began to produce and sell increasing quantities of machines and made many exorbitant claims about the cure of tuberculosis and cancer. Neon glow tubes were used to prove the presence of electromagnetic radiation, in addition to sometimes impressing patients with the marvellous properties of shortwaves that could light the tube without contact.
With over-enthusiasm and lack of precaution, moderate and occasionally severe burns resulted until the circuit and electrode designs were improved. The first electrodes were bare capacitive plates, and later became coated with thick glass shoes with considerable air spacing.
Riviere was the first to use high-frequency current to treat skin cancer in 1900, but the voltage was too low to destroy the cells. De Keating-Hart was the first to apply the spark to destroy tumor tissue, during his demonstration at the International Congress of Electrology in Milan, in 1906. While a great battle for recognition for the discovery of the destruction of tumor tissue by high-frequency currents took place between Riviere and de Keating-Hart, R. F. Cook, in New York, accidentally short-circuited the current from a static electricity machine through his fingers.
The resultant tissue destruction gave him the idea of treating small tumors with a spark of static electricity, and he published his findings unaware that similar work had begun in France [107]. Doyen [37] felt that deeper penetration than that obtained by the electric spark used by de Keating-Hart was needed in order to produce deeper tissue destruction. He believed that normal cells could withstand a temperature of 60° C, but the cancer cells would die at a temperature of 55° C. He also believed that if he could increase the current frequency from 700 kHz to 1 MHz, he would be able to raise tissue temperature to the proper levels and with greater accuracy. He had a manufacturer build such a generator with a small condensor, a resonating coil, and a rotating spark gap. One electrode from the generator was applied to the patient through a moist pad while the other electrode was used for contact with the tissue to be destroyed, resulting in coagulation at a depth of 5 to 8 mm after only two minutes of contact. A survey of work prior to 1920 on treatment of tumors by radio frequency energy was summarized by Rohdenburg and Prime [148], whose own work involved the treatment of spontaneous tumors in mice by X-rays alone, diathermy alone, and a combination of the two. Their work showed that compared with controls, tumors treated with diathermy or X-ray radiation alone showed inhibition, or aggression of growth, while growth was significantly retarded, when the tumors were treated by the combined agents. With 100-MHz shortwave diathermy, the clinical applications of diathermy as an adjunctive treatment of cancer continued with the use of high-frequency generators.
1920’s-1930’s
Work during the period between the 1920's and 1930's is well-summarized by Arons and Sokolov [11]. Although Rohdenburg and Prime [148] contended that combined diathermy and X-ray treatments are required for satisfactory results, Liebesny [108] was able to eradicate carcinoma in mice by using diathermy alone.
With the introduction of shortwave and ultra-shortwave radio-frequency apparatus, Schereschewsky [151] was often able to inhibit the growth of transplanted carcinomas in mice, and in some cases to completely eradicate tumors by treating mice with ultra-shortwaves of 3-m wavelength.
Pflomm [138] was able to inhibit the growth of Jenson-rat sarcoma by shortwave treatments at 4.5-m wavelengths.
Some researchers, for example Reiter [144], after experimenting with shortwaves varying from 3 to 15 m in wavelength, stated that there is a specific biological effect associated with wavelength. He reported that diathermy at 3.5 m was the most efficacious in the treatment of tumors.
He excluded elevated temperature as a possible factor in his interpretation of specific biologic action. Roffo [147] demonstrated that waves ranging from 0.58 to 6.75 m can inhibit the growth of rat sarcoma in vitro, but not that of an embryonic chicken heart. Hill [75] showed that exposure to ultra-shortwave elevation of temperature was insufficient by itself to be tumoricidal, but Mortimer and Osborne [125] believed that heating alone is responsible for evidence that the growth of Ehrlich mouse sarcoma in vitro was retarded when exposed to 3.5-m waves. Eidinow [39] held that there is no specific action of ultra-shortwaves of 3-4-m wavelength, and stated that they act the same way as diathermy currents of longer wavelengths by simply heating the tissues.
Schliephake [152] treated carcinoma of the uterus by a combination of shortwaves and X-rays; he observed after several treatments a marked disintegration of the carcinomatous tissue, but, after suspending treatment for a period of several weeks, malignant growth recurred. Fuchs [58] reported retardation of tumor growth after low-power shortwave exposures, in which heating was negligible, as an adjunct to X-ray therapy. Arons and Sokolov [11] conducted a series of experiments based on the premise of atherinal properties of shortwave therapy in which the temperature in the region treated was not allowed to rise above 26-27°C. They used shortwaves of 6-m wavelength in combination with X-rays to treat 30 cases of human malignancy, including carcinoma of the oral cavity, the larynx, the epigastrium, the uterus, and the rectum. At the time of their report, they could not form definite conclusions concerning the increase of radiosensitivity of the tumors treated by the shortwaves. They stated, however, that the method was qf value in that there was no aggravation or stimulated growth of neoplastic tissue in any of their cases, and that there was a lessening of skin injury by the X-rays. They also reported other benefits of the treatment: post-operative suppuration was inhibited, and an analgesic effect was often observed during the course of treatment.
H. J. Johnson [87], using more precise qualitative methods than those employed by other investigators, reported on the action of shortwaves on transplanted tumors in vivo and in vitro. He developed a technique for continuously measuring elevated temperatures in •tumors during exposure, studied the thermal sensitivity of the Jenson-rat sarcoma and the Walker-rat Carcinoma-256 over a range of temperatures (43.5-47°C). Johnson found that the exposure durations required to produce a 50-percent regression of the Walker-rat Carcinoma-256 at 47,45, and 43.5°C were, respectively, 45 min, 1.5 h, and 6 h. Exposure durations for 50-percent regressions of the Jenson-rat sarcoma at the same set of temperatures were 25 min, 1 h, and 3 h.
Johnson measured temperatures via thermocouples embedded in hypodermic needles; he tried to eliminate coupling of high-frequency currents by using a tuning process.
Considerable problems were encountered with wave trapping by thermocouples under certain conditions, but he was able to obtain reliable temperature measurements.
Despite the early reports of successful use of shortwaves to control malignancies in the laboratory and in the clinic, the methodology was never widely adopted in practice until recently, as discussed in Section III.
II. Medical Applications at Microwave Frequencies
During the late 1930's and early 1940's, there was growing interest in the use of even shorter wavelengths of RF fields for therapeutic purposes. Williams [178] reported that waves of a few centimeters could be focused, and Southworth [163] pointed out that such waves can be directed through hollow conducting tubes (waveguides).
The proposal to use microwaves for therapeutic purposes originated in Germany when Hollman [79] (in 1938-1939) discussed the possibility of therapeutic applications of 25cm waves; he predicted that the waves could be focused to produce heating of the deep tissues without excessive heating of the skin. Similar predictions were made shortly afterward by Hemingway and Stenstrom [74] in the United States. The lack of hardware during the late 1930's prevented development and clinical application of these concepts, and diathermy continued to be applied at frequencies below 100 MHz.
In 1938, the magnetron tube was developed at Bell Laboratories, but the available power it generated was only 2-3 W. Later that year, RCA developed a magnetron capable of generating 20 Wand promised that 100 W could be produced. In 1939, the klystron tube was developed at Stanford University, and promises were made that the tube could soon be used for therapeutic purposes.
Suddenly, at this time when tubes of sufficient power for therapeutic application were known to exist, they all became mysteriously unavailable. It was not until the secret of radar was finally revealed that the medical community realized all such tubes hadl become frozen for military use during World War II. After the war, a magnetron tube developed at M.I.T., capable of generating 400 W at 3000 MHz was available for medical use. In June, 1946, Raytheon Company supplied such a device to the Mayo Clinic for medical research. With the new equipment, therapeutic application of microwaves began at the Mayo Clinic in 1946 [96], [97]. This application involved exposure of laboratory animals to 3000-MHz fields at an output power of 65 W. Temperature distributions in thighs of experimental dogs were measured by thermocouples before and after irradiation. In this work (thermocouples were removed during periods of irradiation), it was demonstrated that deep tissues could be heated, resulting in a number of physiological responses, including an increased blood flow to the treated area. But, as in the case of shortwave diathermy, it was noted that the average elevation of temperature under microwave diathermy was greater in the skin and subcutaneous fat than it was in deeper muscular tissues, although the final temperature in the muscle tissue was higher than that obtained with sources in earlier use.
This work launched the use of microwave diathermy for application in physical medicine. The focusing characteristic of microwaves at that time was believed to be advantageous in that it provided a means of achieving a wide variety of heating patterns with improved flexibility in
therapeutic applications. The fact that the patient was completely free to .move away from the director at any time, and the freedom from pads, encumbering cables, and towelling commonly used with shortwave diathermy were considered distinct advantages. The experimental results seemed to indicate that true deep heating was achieved without undue heating of the cutaneous surface. It must be remembered, however, that these conclusions were based on the use of dogs which have thinner layers of subcutaneous fat and muscle than humans. This new microwave modality gained further credance from dielectric data published as a result of World War II research at the Massachusetts Institute of Technology. The data indicated that the absorption of microwaves at a frequency of 2450 MHz in water at 100° F was in the order of 7000 times greater than the absorption at the commonly used shortwave diathermy of 27 MHz. As a result, in 1946, the Federal Communications Commission assigned the frequency of 2450 MHz to physical medicine based on its alleged superiority in therapeutic value. This is a classic example of how the historic lack of engineering in medicine has prolonged ill-conceived practices not only in medicine, but also in nonrelated industrial applications. The research teams did not consider the fact that the electrical properties and geometry of tissues, wavelength, and electrical skin depth in the tissues, far outweigh the absorption and focusing characteristics of waves in the generation of desirable therapeutic heating patterns. Until the recent popularity of treatment of tumors by microwaves within the last
5 years, there was no commercial microwave diathermy equipment available in the United States, other than the same 2450-MHz apparatus that was conceived in 1947. As a matter of fact, all of the microwave ovens and many of the industrial food processing units being manufactured and used today operate on 2450 MHz, based on the historic frequency allocation.
The microwave diathermy apparatus, approved by the Council on Physical Medicine of the American Medical Association, in December, 1947, and manufactured by Raytheon Company, was known as the Raytheon microthermo. It generated continuous-wave energy in an air-cooled magnetron oscillator tube at a frequency of 2400-2500MHz or a wavelength of approximately 12.2 cm. The energy, variable from 0-125 W, was applied to the patient by one of four possible directors designated A, B, C, or D.
The first three, which were the most popular, are shown in Fig. 9. Directors A and B consisted of hemispherical reflectors containing stub antenna sources, while director C consisted of a small 11.5 X 13.3-cm dihedral corner reflector with a 6.4-cm-Iong half-wave dipole source. The percentage of power used was determined by the spacing from the skin surface, which was generally about 2 in. Treatment time varied from 15 to 30 min. This clinical diathermy machine, along with the C director, are of great interest since they were used for most of the early work and a significant amount of later work on the biological effects of microwaves. In fact, they are still being used today for both therapy and experimental work on biological effects in this country and abroad.
In 1948, Osborne and Frederick used the newly developed machine, with a 60-80 W output for 20 min, to expose the leg muscle of the dog, the frontal sinus of the dog, and the first recorded experiments on the human thigh. In contrast to the results obtained earlier by Krusen and Leden, the newer investigation showed that both the temperature change and the final temperature decreased with penetration in the dog's thigh with an average temperature of 40.1°C, 2 in deep. When the surface of the dog's thigh was cooled by forced air, however, the temperature in the subcutaneous tissues was less than in the deeper muscle tissues. The investigation showed no evidence of damage to the dog's vitreous body after exposure to the microwave radiation. The maximal temperature in the muscle of the thigh was 40.1°C.
Worden et ala [179] found, in 1948, that a monopole antenna with a hemispheric reflector, which was energized at 30 W by 2450-MHz energy, resulted in maximal heating of the thighs of dogs after an exposure period of 20 min when the antenna was located 2.5 cm from the surface of the thigh. If the period of exposure was extended to 30 niin, the temperature dropped as a result of a sharp increase in blood flow. This finding was consistent with that found in 1941 by Mittlemann et ala [123]. Worden et ale also carried out comparative studies on the effects of exposing ischemic tissue and tissue with normal circulation to the. same amount of microwave energy over a period of 15 to 20 min. They reported serious damage in ischemic areas even though the recorded temperatures were not any higher than those found in tissues with normal circulation.
In physical medicine, the effects of electromagnetic fields were believed to arise from simple volume heating. When local elevations of temperature are induced in living tissues, many physiological responses occur that are due in part to direct thermalization of tissues and in part to reflexive changes initiated distally by heating of local nerve receptors. One response is an increase in blood flow via vasodilatation. This response is accompanied by increases in capillary pressure, in cellular-membrane permeability, and in metabolic rate. The latter increase can also produce a further increase in tissue temperature.
Siems et ale [162] performed comparative studies of the effect of shortwave and microwave diathermy on blood flow. Their experiments clearly demonstrated that shortwave and microwave diathermy were equally effective in producing increased blood flow in the extremities of normal
dogs. A number of such experiments were carried out, sometimes with conflicting results. Finally, to resolve the conflict, Richardson et ala [146] carried out research on the relation between deep-tissue temperature and blood flow during irradiation of the gastrocnemius muscles of dogs by shortwave and microwave diathermy. They found with both modalities that it was necessary to increase temperatures at the I-em depth in an extremity of the dog to a level of 42-43°C before a consistent increase in blood flow occurred in the femoral artery. The increase in blood flow was sufficient to diminish the temperature by 3° after once reaching a critical temperature. These results are consistent with the findings of Mittlemann et ale [123], and have been observed subsequently by many researchers and clinicians.
1950
After 1950, and until 1965, research on the use of microwave diathermy in physical medicine expanded significantly.
Clinical and experimental studies were much more predominant than any quantitative work on dosimetry. Gessler, McCarty, and Parkinson [64] appear to be the first group of physicians to use RF energy at microwave frequencies in the experimental treatment of cancer in 1950. They were able to eradicate spontaneous mammary Carcinoma in C3H mice solely by microwave irradiation at 2450 MHz. Five years later, Allen [2] eradicated Crocker sarcoma 39 in rats by combining 1500-2000 r X-rays and 12.5-cm microwaves; the animals were exposed to microwaves 10-20 min, and a peak temperature of 42°C was recorded in the tumors. Crile [27] reported that growth of tumors in dogs and human beings was controlled by 2450MHz microwave diathermy and X-irradiation in combination.
Crile noted, in 1962, that prolonged elevation of temperature in certain cancers at levels between 42 and 50°C selectively destroyed tumors without damaging normal tissues. He concluded that it was a• secondary inflammatory reaction, rather than a primary elevation of temperature, that destroyed the tumors. Two years later, Cater, Silver, and Watkinson [20] reported that combined therapy of 2620 r (220-Kv X-rays) and subsequent 10-cm microwave irradiation of the tumor (47°C for 8 to 10 min) cured some rats of hepatoma 223 transplanted to the leg. The investigators noted that there were no long-term survivors treated by radiation alone or by diathermy alone; tumors were smaller and average survival time was significantly longer in rats treated by the combined therapy. In the same year, Moressi [124] reported that mortality patterns were essentially identical in mouse sarcoma 180 cells exposed to 2450-MHz microwaves and in conventionally heated controls held at the same temperatures over a range of 43-48°C. He found that malignant-cell decay was highly temperature-dependent, as indicated by the “Spontaneous" destruction of cellular material. His investigation also showed that temperature deviations no greater than 1°C, if undetected, can lead to erroneous interpretations, prompting him to write:
"One may critically question the role of unrecognized temperature discrepancies in many of the previously reported studies in which gross results seemed to indicate the presence of a non-thermal factor. Temperature regulation is thus a major concern in investigations where cellular destruction is involved [124]."
III. GROWING INTEREST IN RF HYPERTHERMIA AND CANCER
Although the use of microwaves in therapeutic heating gained in popularity in the 1950's and early 1960's, interest in the use of shortwaves also continued. Birkner and Wachsmann [15] reported regressions and cures in skin carcinoma of patients exposed to shortwaves and X-rays in combination. Exposure of each of the 82 patients for a period of 2.5 h to 6-m shortwaves (tumor temperatures of 42-44°C) alone produced regressions but not cures. When shortwave exposures were combined with X-irradiation, however, some cures were observed. Fuchs [59] reported good clinical results when 6-m shortwave exposures of 10-20 min durations were followed by X-irradiation. He claimed that the good clinical results arose from increased radiosensitivity incident to hyperaemia and to acceleration of metabolism.
In addition to the use of combined RF-field and X-ray therapy, interest developed in the use of microwaves in selective heating of tumors to provide more effective therapy in conjunction with injected radioactive materials and chemotherapy. Copeland and Michaelson [26] reported that the heating of Walker carcinoma 256 by selective radiation (2800-MHz microwaves at 260 mW/cm2 for 5 min) induced a substantial increase in the amount of intravenously injected 1133 fibrinogen that was localized in the tumor. They pointed out that this tumor-heating technique could potentially increase tumor radiation therapy dose from 1133 fibrinogen by 400 percent.
Zimmer et ale [181] reported the use of selective electromagnetic heating in tumors of animals in deep hypothermia to enhance the action of chemotherapy. They treated spontaneous mammary tumors in C3H mice and induced mammary tumors in Sprague-Dawley rats, and found that in 20 control mice there were no spontaneous regressions of tumors, and in 20 mice treated with chemotherapy only, two animals showed regression of tumors with a regression time of 10 days. Only one tumor in the group treated by differential hyperthemia regressed after seven days. In the group of 20 mice treated both by differential hyperthermia and by chemotherapy in combination, 17 animals exhibited regression of tumors after 55 ±25 days. Similar results were obtained from the rats; all 10 animals exposed to S-band fields (2.45 GHz) exhibited regression of tumors; the average regression time was 22 days.
Overgaard and Overgaard [132] provided an excellent review and reported on extensive and well-carried-out experiments on 1200 mice in their laboratory, where transplanted tumors in the mice were permanently cured without damage to surrounding tissues by treatment with 27.12MHz shortwaves. They used a special, field-nonperturbing thermocouple that could be embedded in a tumor to provide automatic regulation of the shortwave output. Thus, it was possible to maintain desired temperature continuously with a variation of about O.l°C. With these carefully controlled elevations in the range of 41.5 to 43.5°C, they were able to work out a quantitative relation between temperature and exposure time for curing the transplanted tumors.
In their analysis, Overgaard and Overgaard showed that the thermalizing treatment induced histological changes in the tumor cells without damaging stomal and vascular cells in the tumor or in the surrounding normal tissue. Immediately after treatment, definite changes were revealed in the mitochondria and lysosomes in the tumor cells. The magnitude of these changes was directly related to the elevation of temperature, and became more pronounced within a few hours or days. The authors noted changes in the nuclei of the tumor cells and in the chromosomal and nucleolar chromatin within the first few hours after exposure. They observed severe injury in all tumor cells 24 h after exposure to a curative dose. Through histological and biochemical observations, the authors obtained clues that allowed them to assume that the direct effect of the heat was a selective activation of the acid hydrolases localized in the lysosomes of the tumor cells.
In later work, Overgaard and Overgaard [133] found that the addition of a small dose of localized X-radiation produced a highly significant intensification of the tumoreradicating effect. They found that successive application of heat and X-rays, both at levels substantially smaller than those required in isolation to produce cures, produced a larger number of total cures. They also noted that intervals as long as 24 h between applications did not appreciably alter the curative effect.
From the mid-1970's on, interest in use of RF fields, either alone or in combination with radiation, increased substantially; a large number of favorable reports on the use of combined therapy has appeared in symposia proceedings and publications. Among these are the Proceedings
of the First and Second International Symposia on Cancer Therapy by Hyperthermia and Irradiation [4], [166]; a Special Issue of IEEE TRANSACTIONS MICROWAVE THEORY AND TECHNIQUES on microwaves and medicine, with accent on the application of RF energy to cancer treatment [82]; a special Radiation and Environmental Biophysics issue on hyperthermia in cancer therapy [143]; the Third International Symposium on Cancer Therapy by Hyperthermia, Drugs, and Radiation [172]; a Special Issue of the Journal of Microwave Power on Electromagnetic Hyperthermia [89]; and the Annals of the New York Academy of Science, Thermal Characteristics of Tumors: Applications in Detection and Treatments [6]. In addition, four new textbooks, Lehmann [105], Storm [165], Hahn [73], and Gautherie and Albert [63] cover the subject in great detail.
Some examples of more recent applications of submicrowave RF fields are in the reports of von Ardenne [175], Overgaard [131], Kim et ale [94], [95], LeVeen [106], Storm et ale [164], and Gibbs [65]. Continuing success is reported in the use of microwave hyperthermia as an adjunct in the treatment of tumor. Szmigielski et ale [171] reported prolonged survival of mice bearing Sarcoma-180 tumors after irradiation by 3000-MHz microwaves such that rectal temperature increased by 3-4°C. The inhibitory effects of microwave hyperthermia was enhanced by simultaneous treatment of the mice with interferon and interferon inducers.
Mendecki et ale [115] completely eradicated transplanted mammary adenocarcinoma in C3H mice and, in several clinical cases, obtained favorable results in the treatment of basal-cell carcinoma, malignant melanoma, and skin metastases of carcinoma of the breast by both 2450-MHz and 915-MHz fields. In these studies, the temperature of the tumors was raised to a temperature between 42.5 and 43°C. Nelson and Holt [127] and Hornback et ale [80], [81] successfully treated cancers in patients by combined therapy with 433-MHz fields and ionizing radiation.
More recent clinical successes with microwave hyperthermia have been reported by Gibbs [65] and Perez [136]. Interstitial application of low-frequency energy (500-kHz) has also been successfully used in the treatment of tumors [25].
IV. BIOLOGICAL HAZARDS
Since the earliest use of RF energy for medical applications it has been known that excessive heating of the tissue can be hazardous and cause injury. However, there also has been interest in and concern for athermal effects. Arguments in support of and against the thesis of athermal effects developed during the early history of the therapeutic application of RF waves. In addition to the claimed frequency-specific effects in shortwave treatment of tumors, Danilewsky and Worobjew [32] demonstrated that contractions by frog nerve-muscle preparations increased in amplitude
when high-frequency currents were applied along with minimal faradic stimulation. When the high-frequency currents were removed, the excitability of the nerve rapidly returned to its original value. With increasing current (at 0.5-1.0 MHz), a point was reached at which excitability was depressed. This same phenomenon of altered nerve-muscle excitability was also obtained by irradiating the sciatic nerve of a warm-blooded animal.
Audiat [12] asserted that, because excitability of the nerve-muscle preparation diminished under the action of RF waves, it had to be a "specific" effect, since heating supposedly would have an opposite effect. It was also claimed by Delherm and Fischgold [36] that high-frequency currents diminished excitability of the nerve-muscle preparation in a manner similar to that produced by the anodic effect of a direct current. Later, it was shown by Weissenberg [176] that interrupted high-frequency current applied to a nerve-muscle preparation of a frog showed stimulating effects similar to those obtained by a pulsating dc current." It was postulated that the nerve rectified a small portion of the applied current. Pflomm [138] stated that when a frog's heart was placed in a shortwave field, the beat became slower and that contractions lessened with the diastolic beat finally ceasing; but if the field were switched off, the heart gradually resumed its activity. Hill and Taylor [76], on the other hand, repeated Pflomm's work, showing that weak, high-frequency fields at wavelengths of 600, 22, and 6 m would increase the excitability of a nerve-muscle preparation, whereas stronger currents produced a depression of excitability. They showed that similar effects could be produced by a hot wire placed near the nerve and concluded that the mode of action of the high-frequency current on the nerve-muscle preparation is thermal. These researchers also demonstrated that the effects observed by Pflomm on the frog's heart were identical to that obtained when the frog's heart was warmed by conventional means.
The first study on the effects of microwaves on living mammalian tissue was conducted by the Armed Forces in answer to a morale problem by Daily [29], Follis [45], and Lidman and Cohn [109]. The studies were meant to dispel fears of possible ill effects of EM radiation upon personnel connected with radar work. The reports, which indicated no ill effects, were concerned only with the exposure of animals to radar pulses. Later, however, Richardson et ale [145] were able to induce lenticular opacities in the eyes of rabbits and dogs exposed at a distance of 5.08 cm. Daily et ale [31] also were able to produce cataracts and other eye-tissue damage in rabbits, and Imig et ale [83] were able to produce testicular degeneration in rats exposed to the same generator. Oldendorf [128] performed one of the earliest studies on the effect of microwaves on the CNS.
The results, thermal in origin, showed that focal coagulation necrosis could be produced in the brain of rabbits exposed to 2450 MHz. This resulted in irritability and altered equilibrium. Daily et ale [30] also were able to produce cataracts in the eyes of rabbits exposed to the 2450-MHz diathermy source. During and after 1950, there was a considerable amount of research done in the use of the 2450-MHz diathermy apparatus. A microwave-induced
human cataract (first reported by Hirsch [77]) was found in the eye of a microwave technician who habitually looked into a microwave horn-type antenna at close range while performing certain tests.
After 1950, research on the' use of microwaves for diathermy and also on hazardous biological effects mushroomed. Though the most obvious effects of microwaves were thermal in nature, evidence was sought on the possibility of nonthermal effects.
The Armed Forces became involved in the problem of radiation safety in 1956, in connection with radar personnel.
The Department of Defense, through the United States Air Force and the Tri-Service ad hoc Committee, undertook a comprehensive analysis of the biological aspects and associated hazards of exposure to microwave radiation. A $13 million study was launched, and biological effects due to a wide range of frequencies and power levels were noted.
The results of these studies were reported and documented, during symposia held in 1957, 1958, 1959, and 1960 (Pattishall [134], [135], Susskind [168], Peyton [137]). Most of the work indicated that the major effects of microwaves in biological tissues was due either to localized or to general hyperthermia or elevation of temperature in the tissues, producing the greatest danger to areas with poor or no blood circulation, such as the eyes and testicles.
Michaelson et ale [118] and Michaelson [120], [121] showed that sufficient power and exposure time could produce breakdown of thermal regulation in the biological system resulting in death. He also demonstrated effects of radiation on blood composition, where some blood-cell levels could be increased and other decreased after exposure of an animal to microwaves. Effects were demonstrated on the thyroid, immune response, endocrine response, cardiovascular system, and central nervous system. Effects were observed on the biological systems' immunity and tolerance to ionizing radiation. The possibility that microwaves may interact with biological material without the production of heat was pointed out, but most of the research results obtained in this country at that time did not support this. As a result of the studies, the previously recommended safe exposure level of 10 mW/cnr (discussed in Section V) continued to be used.
The work being done in the Soviet Union, however, indicated that effects on the central nervous system were taking place at nonthermal levels below 10 mW/cm2
As a result of their work, the Soviet GOST, in 1958, set their safety level for continuous exposure three orders of magnitude lower (10 JLW/cm2 ) than that which was later set in the United States. Some scientists in the United States stated that Soviet studies were oriented toward the Pavlovian
concept of "Nervism," which presumes that all body functions are influenced by the central nervous system. Since experimental support for the approach was obtained by conditional response studies, it was criticized by many U.S. researchers involved in the Tri-Service Program. The work was also criticized for the limited statistical analysis of data, inadequate controls, and difficulty in objective interpretation of the findings (see, for example, Michaelson et ale [118] and Frey [55]).
There were a few other American researchers, however, who believed that there was a possibility for the existence of deleterious nonthermal effects (Frey [55]). Complete references on work since 1950 are too numerous to discuss completely here, but they are well-documented with comprehensive reviews, beginning with the records of the Congressional Hearings on the Radiation Control for Health and Safety Act of 1967 [5]. In particular, the discussion by Michaelson et ale [119]'gave an excellent survey of the work prior to 1968. Examples of studies concerning dosimetry
and modes of wave propagation in the tissues include work done by Schwan [157], [159], [160], Anne et ale [7], [8], and Livenson [111]. Examples of studies done on thermal effects include work done by Michaelson et ale [116]-[119], Carpenter and Van Ummersen [19], and Ely et ale [41],
while examples of work done on nonthermal effects involve Susskip.d [168], Schwan [159], Kholodov [91]-[93], Presman [140], [141],' Livshits [112], and Frey [51], [52], [54], [55]. A book by Presman [142] of the Soviet Union, translated into English, provides an excellent treatment of Soviet work on
both thermal and nonthermal. effects. One of the more curious effects observed by radar technicians during World War II was the microwave hearing phenomenon first noted in an electronic equipment advertisement (Airborn Instruments Laboratory, 1956) and investigated in great detail by Frey [51]-[53], [56]. The fact that the mechanism of the phenomenon was not known for nearly three decades attests to the historic absence of adequate attention by engineers and physical scientists to the bioelectromagnetics field. Actually, the necessary work required to explain the phenomenon in terms of thermo elastic acoustic disturbances was done for nonbiological materials exposed to EM waves by White [177]. This phenomenon was not related to the hearing effect until 11 years later by Foster and Finch [46]. Detailed reviews of the work relating to this problem have been made by Lin [110] and Chou and Guy [23].
Another bizarre interaction that still defies explanation is the observance of effects in biological preparations only when they are exposed to certain "windows" of modulation frequency in the ELF band and low-level power density (Bawin et ale [13], Blackman et ale [16]). Though the results are controversial, the fact that they have been observed by multiple investigators has enhanced the credibility of the findings.
V. Dosimetry and Quantifications of Effects
Between 1931 and 1941, there were many basic problems in the use of radiofrequency energy for effective therapeutic heating of tissues. Most of these problems arose because investigators were not able to quantify the actual rate of energy absorption by tissues during treatment. The results of uncontrolled experiments resulted in contradictory statements in the medical literature. The various shortwave generators produced by different manufacturers had variable outputs. It was implied through advertisements that the heating of deeper tissues would be enhanced with greater output power of the generating equipment.
Since the extent of heating of tissues seemed to vary considerably with frequency, even with the same apparent output power of the various devices, many researchers jumped to the conclusion that there were selective therapeutic properties associated with specific wavelengths.
A research team consisting of engineers and physicians (Mittlemann, Osborne, and Coulter [123]) measured elevations of temperature in vivo in tissues as a function of time rates and quantities of energy absorption; they presciently recognized that quantities of absorbed energy are superior to the output power of the diathermy applicator and the exposure level as dosimetric indices. The team instrumented a shortwave diathermy generator so that the energy absorbed by a patient under treatment could be measured to levels within 5 percent. As expected, the power level of absorbed energy was highly correlated with the rate of temperature elevation of the tissues. The results interrelated absorbed energy, elevations of temperature, and duration of treatment (i.e., watts per 1000 cc of tissue for a O.I°F elevation per minute). This work made use, for the first time, of volume-normalized rates of energy absorption in units (Wjliter) closely related to the Wjkg now widely used to index the RF dose rate, the SAR. The results of the energy-absorption measurements agreed closely with theory.
The amount of energy absorbed per unit volume that raised the tissue temperature to a certain extent in a given period of time was virtually the same in all of their tests.
Mittlemann et ale [123] conducted another series of measurements in which a patient was exposed to fields of differing wavelengths under differing conditions of exposure. Their results indicated that the delta T per minute was proportional to the quantity of energy absorbed by the patient.
The work by Mittlemann et ale [123] clearly demonstrated that the averaged extent of tissue heating is dependent on the rate of energy absorption and not on the wavelength of the field for similar ratios of deep-to-superficial heating. Their work also indicated that there was a marked difference in the character of the temperature-time curves at high and low levels of power. At levels of power below 100 W (calculated SAR = 33 to 42 Wjkg), temperature in the deep tissue was noted to rise along a straight line until near the termination of the 20-min exposure period. When the SAR exceeded 42 Wjkg, the final temperature was lower than the earlier peak temperature, due to vasodilation, which rapidly cooled the volume of exposed tissue by circulatory convection.
During the first ten years of development and use of shortwave diathermy, most research consisted of measuring the temperatures of superficial and deep tissues of both animal and human subjects exposed to capacitive- and inductive-type applicators, the generator wavelengths of which varied from 6 to 24 m. The only dosimetric index at this earlier time was the power level of a source or a temperature measurement in tissues. A number of researchers, as a result of their observations of varying T 's in exposed tissues in association with different wavelengths, concluded that absorption characteristics are wavelength specific. Others, however, such as Osborne and Coulter [129], concluded that the variations were more dependent on electrode configuration and spacing and the geometry of the tissue being heated than on frequency. These early researchers also observed that it was difficult to produce therapeutic elevations to 42-45°C in deeper tissues, such as muscle and bone marrow, without adversely affecting the skin and other more superficial tissues.
Significant research to quantify various biological effects of electromagnetic field was done by Schwan [154]-[158] at the University of Pennsylvania. Schwan's work on dielectric properties of biological tissues and on the influence of tissue geometries on scattering properties deserves considerable attention. Schwan demonstrated theoretically that microwave irradiation at a frequency of 2450 MHz is not therapeutically advantageous because of several major deficiencies,
including: 1) excessive heating of subcutaneous fat by standing waves, 2) poor penetration into muscle tissue because of poor ,penetration, and 3) poor control of the distribution of energy absorption in the patient because of large variations in electrical thickness of tissues (compared with the wavelength of subcutaneous tissues). He recommended that frequencies be reduced to 900 MHz and lower.
During the period of concern about biological effects the therapeutic applications of microwaves continued first at a slow pace but then accelerated due to the popularity of heat therapy as an adjuvent for the treatment of cancer. Lehmann et ale [98]-[102] and Guy [67] experimentally verified Schwan's earlier theoretical prediction that irradiation at 900 MHz or below can produce more determinate therapeutic patterns than those obtained with 2450-MHz fields. Since 1966, LehmaQn et ale [104], deLateur [35], Guy [68], [69], and Guy et ale [70] have developed and clinically tested extant 915-MHz equipment.
Recently, there have been considerable advances in the design, efficacy, and safety of both shortwave- and microwave- hyperthermia applicators and systems (Christiansen and Durney [24], Kantor [90], Cheung et ale [22]). Work in the characterization of biophysical properties of normal tissues under RF irradiation is being extended to include neoplastic tissue by Foster et ale [47], Burdette [18], and Stuchly et ale [167].
Much of the past research involved the application of radiation fields to various small animals and noting such qualitative effects as tissue changes. Although the TriService studies in the later 1950's provided a large amount of qualitative data, they did not contribute much to a full quantitative understanding of either the effects of electromagnetic fields on human tissues or the effects of human tissues on electromagnetic fields. A large portion of the work was devoted to establishing the electromagnetic power densities in the vicinity of various radar sources, exposing the animals or biological tissues to microwave sources and observing the resulting changes in the tissues, and exposing crude phantom-tissue models to microwaves and observing the temperature changes. In most cases, the magnitude of the applied field was based on predictions or measurements for an undisturbed field condition in front of a radar source or in a test chamber. The absorption, diffraction, and scattering effects of the test animal or specimen on the applied field was usually not accounted for. The fact that these effects vary greatly from animal to animal, and especially from animal to man, was ignored. Therefore, the induced changes in tissues and electromagnetic-field tolerance levels were invariably related to an undisturbed field of radar source rather than the actual field strengths present in the tissues. The latter criterion is paramount if the effects observed in animals or tissue samples are to be extrapolated to mankind. As a result of this qualitative approach, equations, empirical rules, or data for predicting reliably the electromagnetic fields and the associated thermal and nonthermal effects anywhere in the human body for a given incident energy source were generally unavailable.
Anne [7], however, did derive approximate bulk absorption characteristics for the human body for a given incident plane-wave field. This theoretical work was based on an analysis of a perfect spherical' shape, with the dielectric characteristics of human tissues. The experimental work was based on a phantom model consisting of a large bottle filled with a dioxane-water mixture. The dielectric properties of the liquid were adjusted to correspond to those of human muscle. In addition to medical applications, work was also directed to the understanding of potential biological
hazards and methods for quantifying interaction of electromagnetic fields with biological tissues. In the late 1950's, the possibility of producing high field intensity, but nonthermal, "pearl chain" effects in biological fluids containing suspended small particles of biological material of differing dielectric properties was demonstrated (Saito [149], Furedi et ale [60], [61], Schwan [159]). Studies began in the early 1960's on determining the relationship of exposure frequency, subject size, and subject shape with energy coupling (Anne [7], [9], Anne et ale [8]). Analyses were performed with prolate spheroidal tissue models using static solutions to determine low-frequency quasi-static field coupling and spheres using the Mie theory to determine plane-wave field-coupling characteristics with the bodies of humans. The studies with the spheres indicated that the absorption cross section varied markedly with frequency with sharp minima and maxima. Franke [49], of the U.S.S.R., in 1961, was the first to simulate the human form with cylinders and prolate spheroids and to expose to different field polarizations to calculate the absorbed energy. Franke was the first to demonstrate the sharp differences in absorbed energy as a function of polarization and to demonstrate resonance in a human-like model.
Franke also demonstrated the dependence of absorption on the square of frequency below resonance and the fact that in this frequency raI}ge the absorption due to electric field exposure could be calculated separately from that due to magnetic-field exposures.
After the mid-1960's, experimental phantom models of various tissue were developed and used for experimentally verifying the theoretical analysis and determining field coupling and absorption characteristics for more complex tissue structures not amenable to theoretical analysis. From the late 1960's until the present, thermography has played a powerful role in measuring the EM-field-induced temperature changes in both phantom and actual biological tissues, allowing for a rapid and accurate quantification of the absorbed energy and electric-field distributions within the tissues. Both theoretical work and the development of new instrumentation increased substantially in the 1970's.
Complex spherical models of the human head consisting of a core of brain tissue and spherical shells simulating the skull and the scalp indicated that hot spots or localized regions of high energy absorption could occur in the center of the brain with magnitudes much higher than observed at
the surface of the head due to the focusing of energy by the high dielectric constant and spherical shape of the head (Shapiro et ale [161], Guy [71]). More extensive analyses using spherical, prolate spherical, and ellipsoidal models created a much better understanding of the absorbed energy
patterns in the bodies of man and animals exposed to EM fields (Ho et ale [78], Durney et ale [38], Johnson et ale [86], Massoudi et ale [113], Gandhi [62], Allen et ale [3]).
Theoretical work was being backed up by careful experiments utilizing special temperature-sensing probes composed of microwave transparent materials such as fiber optics and miniature leads of low electrical conductivity (Chen et ale [21], Hagmann et ale [72]). Finite-difference techniques and. other numerical methods are being used in computer programs for calculating EM-field and associated heating patterns in arbitrarily shaped bodies more closely simulating man. Mathematical models were developed to include the effect of cooling mechanisms including blood flow for calculating steady-state temperatures in various parts of the body, including critical organs such as
the eyes and the brain (Emery et ale [42], [43]). Theoretical analyses coupled with animal experiments indicated that the long-known but unexplained microwave hearing effect where individuals exposed to pulse radars could hear clicks and buzzing sounds was due to the conversion of microwave pulses to heat in the tissues• of the head. The effect previously was thought to be a nonthermal effect since the threshold energy of a microwave pulse required to elicit the effect is sufficient to produce a temperature rise of only 10-50 C. Though there were a number of theoretical analyses suggesting the possibility of low-level nonthermal effects, the existence of such effects were still under dispute (Vogelhut [173], Grodsky [66], Frohlich [57]).
VI. SAFE EXPOSURE STANDARDS
In 1953, Schwan recommended that microwave radiation of 10 mWIsqcm be accepted as a tolerance dose. Five years later, however, the Soviet Union promulgated an occupational standard limiting microwave exposure to only 10 uWIsqcm. Subsequently, after a review of all the experimental
data on animal exposure at that time, it was the conclusion of various American investigators that it required exposure levels in excess of 100 mWIcnr to produce any effect of biological significance. On this basis, with a safety factor of ten, a maximum safe exposure level of 10 mWIcnr was recommended by the United States of America Standards Institute (USASI) in 1966. The standard specifying only power density was defined to cover the frequency range 10 MHz-100 GHz. Later, the name of USASI was changed to the American National Standards Institute (ANSI), and the ANSI-C95 Committee responsible for the 1966 recommended guidelines continued its work under the chairmanship of Prof. Saul Rosenthal of the Brooklyn Polytechnical Institute (now the Polytechnical Institute of New York). The charter of ANSI required that the exposure guide be in effect for only five years. At the end of five years, ANSI had the choice of three possible actions based on the recommendations of the C95 Committee:
1) reaffirm the guidelines with no change,
2) modify the guidelines based on new information concerning exposure hazards, or
3) withdraw the guidelines.
Anyone of the three actions required a strong consensus by the membership of the C95 Committee. The membership of the Committee is required to be balanced with members representing a) government, b) industry, and c) the general public. The technical work and scientific recommendations concerning guidelines for safe use of radio-frequency electromagnetic fields is carried out by various subcommittees with memberships comprised of scientists with expertise on the particular problem addressed by the subcommittee.
Subcommittee IV has always been responsible for the guidelines pertaining to human health.
In the 1960's, a segment of the population was exposed to excessive X-ray radiation emitted from certain color television sets. This prompted Congress to pass legislation in 1968 to protect the public from all forms of electromagnetic radiation, including microwaves that could be emitted from manufactured electronic equipment. The new law, called the Radiation Control for Health and Safety Act of 1968 [5], appeared simultaneously with the increasing sales of microwave ovens and a growing concern of the great difference between the Soviet and East European occupational
exposure standard and the ANSI standard. This produced an immediate crunch between the microwave oven industry and the government.
The microwave oven industry, represented by the Association of Home Appliance Manufacturers (AHAM), felt that the ovens being manufactured were perfectly safe for mass distribution to the public. They claimed that the oven doors, the part of the oven most susceptible to microwave leakage, were designed to limit microwave radiation values to less than the accepted tolerance level of 10 mW/cm2
It also was stated that the doors were further protected with interlock switches to disable the microwave power source (usually 600-700 W) if the door was inadvertently opened. A government survey, on the other hand, at the time indicated that an alarmingly high percentage of microwave
ovens being used by the public were leaking microwave energy to such an extent that nearby persons could be exposed to energy levels far in excess of 10 mW/cm2
Furthermore, the government was alarmed about the large discrepancy between the established United States and Soviet safety levels and the abundance of Russian literature on the deleterious effects of low-level microwave radiation.
They were also worried about the fact that American scientists did not even agree with each other on where safety levels should be and also the fact that a high percentage of past research results were in doubt due to lack of meaningful dosimetry. Consequently, in the spring of 1970, armed with the new law, the Bureau of Radiological Health set the legal maximum radiation leakage level from microwave ovens to 1 mWIcm2 or less at the time of delivery and no more than 5 mWI cm2 during the lifetime of the oven as measured 5 cm from the surface of any portion of the oven. It should be noted that this was an emission or performance standard based on limiting radiation from a device in contrast to an exposure standard which specifies maximum exposure level for a human subject. By the inverse square dependence of radiation fields, aImWI cm2 emission level 5 cm from the oven would result in a 10 J-LWIcm2 exposure level at 50 cm away.
Since whole-body exposure would require that the subject be 50 cm or more away from the oven, the standard provided the same degree of protection or better for whole-body exposure as the Soviet occupational standard.
The new performance standard resulted in a clamor of protests from AHAM, who claimed that there was no basis for lowering the standard and it could result in prohibitive manufacturing costs. •It was claimed that these restrictions would hinder the widespread use of microwave ovens.
At the beginning of the ANSI C95 IV Subcommittee began a series of meetings to respond to growing criticisms of the 1966 guidelines. The committee was not able to act in time for the required 1971 five-year action on the guidelines, and through much controversy and heated discussions
was forced to reaffirm the 10 mWIcm2 standard in 1974. It was stated that there was insufficient information in the available data base to make any quantitative modification of the guidelines. The guidelines were changed slightly, however, to specify the maximum equivalent rms electric (200 V1m) and magnetic (0.5 Aim) field strengths consistent with values corresponding to a radiation power density of 10 mWIcm2 [10]. The Committee released a publication discussing the problems with the existing data base and recommended the type of research needed for refining the guidelines (Johnson [84], [85]).
With the mushrooming research of the late 1970's providing more quantitative research results, the ANSI C95 Committee (again, three years later tp-an the required time) promulgated new guidelines (ANSI C95.1, 1982) that answered many of the criticisms directed at the old guidelines.
The guidelines, covering a new frequency range of 300 kHz-100 GHz, limited the maximum average rate of absorbed energy in an exposed person to 0.4 WIkg. This was considered safe by a factor of 10 from the 4 WIkg threshold for harmful effects in exposed animals. This basis required that the actual maximum exposure levels change with frequency according to the absorption characteristics of the human body. The guidelines were recommended for both occupational and general population exposures.
In spite of the wave of criticisms from some quarters that the standard was not conservative enough, it became a benchmark for nongovernmental and governmental standards and one international standard. The American Conference of Industrial and Governmental Hygienists have adopted a standard similar to the ANSI standard, except it extended the guidelines set for 300 kHz down to 10 kHz. The Commonwealth of Massachusetts adopted the ANSI standard for occupational exposures but lowered the frequency-dependent exposure level by a factor of five for the general population. The Massachusetts standard was also adopted by Multnomah County, OR.
The International Radiation Protection Association (IRPA, 1984),1 which has members from the Soviet Union and East European countries as well as from the United States and Western countries, recommended the ANSI guidelines for occupational exposures and exposure levels similar to the Massachusetts criteria for the general population.
Currently, the National Institute of Occupational Safety and Health (NIOSH) is seeking agreement on a legal standard for enforcement by the Occupational Safety and Health. Administration (OSHA), and the Environmental Protection Agency (EPA) is in the process of recommending guidelines to various government agencies for limiting exposures of the general population from radio frequency energy emitted by equipment or systems they use or control.
In 2001 the FCC and other PTT’s around the world adopted EMR safety planning levels for new communication links, amateur operations and other communications devices. These are based on frequency of operation, antenna radiation pattern, power output and the proximity of people in both a transient exposure or a long term occupational exposure. The EMR safety guidelines used by Australia’s ACMA in 2001 were correctly frequency dependant only up to 50Mhz, above which their guidelines ignored transmitter frequencies.
VII. PROFESSIONAL SOCIETIES, GOVERNMENTAL ORGANIZATIONS
This document will not be complete without discussing the role professional societies and various government programs have played in shaping the history of the bioelectromagnetics field. The first society dealing extensively with the subject was the American Electrotherapeutic Association, which in 1898 provided a forum for Tesla's lectures on therapeutic applications of RF current (Susskind [169]).
In the early 1930's and later, the American Congress of Physical Medicine devoted considerable attention to the medical applications of radio frequency energy through their journals and international conferences [169]. Many of the research and clinical reports dealing with the subject up until the mid-1960's appeared in physical medicine periodicals such as the American Journal of Physical Medicine and the Archives of Physical Medicine and Rehabilitation; however, on rare occasions the PROCEEDINGS OF THE IEEE and some of the IEEE TRANSACTIONS published articles on the subject. The first engineering organization devoting continuous attention to the field.' was the International Microwave Power Institute (IMPI) founded in 1966. In the following years, IMPI held annual symposia and published a periodical called the Journal of Microwave Power addressing peacetime nonradar and noncommunication applications of microwaves including medical and biological.
The first nonmilitary government laboratory dealing with the bioelectromagnetics field was the Bureau of Radiological Health (BRH), w4ich was given responsibility within the Department of Health, Education, and Welfare (HEW) in 1968 by the Radiation Control for Health and Safety Act to carry out and sponsor research and to develop safety criteria concerning health effects of the radiation emitted by electronic products. BRH began its mission by sponsoring a symposium devoted entirely to the health effects of nonionizing radiation which was the first held in the country since the years of the Tri-Service work. The meeting held in cooperation with the Medical College of Virginia, in Richmond, in 1969, was designed to help HEW evaluate the potential hazards of microwave radiation.
However, the meeting indicated that considerably more scientific information was needed to dispell the differences between two schools of thought: 1) the existing 10 mWIcm2 ANSI standard was adequate or 2) the 1958 10 JLWIcm2 Soviet standard was more realistic. Following the 1968 Radiation Control Act, a committee called the Technical Electronic Product Radiation Safety and Standards Committee (TEPRSSC), comprised of members from industry and the private sector, was formed to advise BRH concerning their work on electronic device safety. Also in the same year, the Electromagnetic Management Advisory Council (ERMAC) was formed under the Office of Telecommunications Policy under the Executive Office of the President to coordinate programs and influence research funding on the biological effects problem by the various governmental agencies. The ERMAC held a number of public meetings over a period of years reviewing the work and making recommendations concerning the research programs of a number of governmental agencies and their contractors.
Later, in 1970, coordination between governmental agencies on the problem increased further in the form of Department of Commerce's Interagency Task Force on Biological Effects of Nonionizing Electromagnetic Radiation (BENER). The same year, the U.S. Navy proposed the construction of a large buried ELF communication antenna in the State of Michigan, which triggered a controversy about possible health side effects that has raged until 1984 with the project stopped by a recent court injunction. The project sought a friendly home in states ranging from the Great Lakes to the Gulf of Mexico.
The public resistance to the project based on fears of health side effects stimulated a large research program by the U.S. Navy for assessing the health effects of ELF fields. This concern about the ELF effects eventually led to similar concern and controversy relating to 60-Hz highvoltage power lines, which in turn stimulated additional funding for research on ELF effects by the Department of Energy (DOE), the Electric Power Research Institute (EPRI), and the Public Health Department of the State of New York.
With the growing concern and controversy, scientific and engineering societies began to take action to educate their members as well as play a part in public education concerning the state of the art of the field. The IEEE MTT Society became involved in the early 1970's by setting up a Technical Committee on the Biological Effects of Microwave Radiation, adding engineering experts on biological effects to their Administrative Committee and in 1971 publishing a Transactions Special Issue devoted entirely to the problem of biological effects of microwaves, with invited papers from researchers from the old Tri-Services group and the group of emerging new researchers involved with the problem. Various agencies in the g9vernment charged with funding scientific research also took action to educate themselves. The National Science Foundation (NSF) held a special workshop at the University of Colorado for assessing priorities and research needs pertaining to the problem in 1971. This set the stage for NSF funding of interdisciplinary research on the subject which coincided with increased funding of interdisciplinary research by many governmental agencies. With the increase in new research results there was a clamor by various professional societies to sponsor sessions in their annual symposia or publish papers in their journals on the latest biological effects research. The U.S. National Committee of URSI began including such papers in their meetings beginning in 1971, the biannual Conference on Precision Electromagnetic Measurements (CPEM) in 1972, and by 1973 the IEEE MTT Society began to compete strongly with IMPI on the number of biological effects papers presented in their annual symposia. The MTT-S Committee on Biological Effects of Microwaves invited biological effects and microwave dosimetry papers for inclusion in the TRANSACTIONS and annual symposia. The year 1972 marked an increasing awareness and concern by the public of nonionizing radiation hazards which stemmed from a number of news and journal articles.
The articles stressed some of the more bizarre reported effects, the lack of knowledge concerning these effects, and the big difference in the world safety standards on nonionizing radiation. A number of these articles were somewhat sensational in nature and out of perspective with true state-of-art and knowledge of the field. The Consumers Union went so far as to recommend against the purchase of a microwave oven if any microwave leakage from it could be detected. The widespread confusion and public misunderstanding arising from the media coverage prompted the IEEE in 1972 to form a Committee on Man and Radiation (COMAR) to respond to irresponsible journalism relating to EM radiation effects in the form of public education and position papers. Meantime, governmental involvement in the problem area increased with the formation of the Environmental Protection Agency (EPA) in 1972. This was not without impacting, however, the newly functioning BRH laboratory, which had built up an interdisciplinary group of engineers and life scientists to carry out research on the problem. By governmental edict, half of the interdisciplinary scientists and engineers of the laboratory transferred to EPA to form another laboratory devoted to the RF-bioeffects research area. The precursor for East-West scientific cooperation on the subject occurred in 1972, with the signing of the agreement between Nixon and Brezhnev, on environmental health exchange.
The East-West cooperation actually began with sponsorship of the First International Symposium on Biological Effects and Health Hazards of Microwave Radiation near Warsaw, in 1973, by the U.S. HEW, the Polish Ministry of Health, and the World Health Organization (WHO). The first dialog and information exchange between the Soviet, East-Bloc and Western-country researchers and public health specialists occurred at this meeting with the results documented in a bound proceedings
[180]. Following the Warsaw meeting, there was an acceleration of bioeffects research in both the U.S. and the U.S.S.R., as well as other countries. This was followed by a formal agreement signed in 1975 between the National Institute of Environmental Sciences for the U.S.A. and the Kiev Marzeev Institute for Communat and General Hygiene representing the U.S.S.R., under the umbrella of the Environmental Health Agreement, to engage in cooperative research and scientific exchange on the microwave biological effects.
In 1974, the International Council on Radiation Protection Measurements (NCRP), an organization previously chartered by Congress for providing ionizing radiation advice and education to the public and the scientific community, expanded their activities to the area of nonionizing radiation and electing a number of scientists and engineers involved with nonionizing radiation to its membership. An NCRP scientific committee was formed to begin work on a report specifying appropriate quantities and units for use in nonionizing radiation research and safety standard work. By 1975, the engineering and scientific community involved with the bioeffects research was frustrated by its need to interact with so many scientific societies and organizations and to monitor so many different journals in order to keep Current with the field. It was agreed by the majority of researchers in the field that the time had come for an annual conference to be established, at which all researchers could gather simultaneously to present their research findings.
It was felt at the time, that URSI provided the best umbrella and resource for holding these meetings, since unlike other organizations such as IMPI and IEEE, it was not a pure engineering group, but included scientists and engineers involved with the broad topic of radioscience on an international scale and, ther~fore, was compatible with their interests. The U.S. National Committee of URSI agreed to include a series on biological effects at its 1975 meeting at Boulder, CO, resulting in more than 100 papers being presented. As a result of the success of the meeting, a similar meeting was held at the USNC/URSI meeting in 1976 (Radio Science, 1978), which set the stage for a full-scale international URSI meeting devoted entirely to the EM bioeffects area in the fall of 1977 at Airlie, VA (Radio Science, 1979). This meeting was significant since it was held with full cooperation from all countries involved in EM bioeffects research including the Soviet Union and the East-Bloc countries. A similar meeting or symposium was held in conjunction with the URSI General Assembly meeting in Helsinki, Finland, in 1978, again involving participation from all countries (Radio Science, 1982).
While most of the attention by the scientific community involved in this work was directed toward the biological side effects of microwave radiation, new interest in the use of radio frequency energy for treatment of cancer was ignited and the First International Symposium on Hyperthermia
in Cancer was held in Roslyn, VA, in 1975, sponsored by the National Cancer Institute and American
College of Radiology. Similar meetings covering cancer treatment by RF energy have continued to the present time, along with meetings held by other groups such as the Radiation Research Society and the Radiation Therapy Oncology Group (RTOG).
The tempo of the public alarm concerning health effects of nonionizing radiation increased substantially following two articles by a well-known writer, Paul Brodeur, in the New Yorker magazine, which emphasized the danger of microwave radiation to the public and claimed that there was a cover-up by the government of these dangers. The articles were followed up by the publication of the book entitled The Zapping of America, in 1977, by the same author.
The bioelectromagnetics research area had matured sufficiently by 1978, so that the large scientific group involved formed their own society, called the Bioelectromagnetics Society (BEMS), and agreed to sponsor all future major symposia on the biological effects and medical applications of nonionizing radiation in the United States. This society held its first meeting in conjunction with the International Antennas and Propagation Symposium at the USNC/URSI meeting in Seattle, in 1979. In the following year, BEMS introduced their quarterly Journal of Bioelectromagnetics and began to hold annual biological effects meetings independent of URSIe Since that time, a number of new societies have formed with attention devoted to specialized areas of bioelectromagnetics, including the Bioelectric Repair and Growth Society (BRAGS) and the Bioelectric Chemistry Society (BES).
About the Primary author
Arthur W. Guy (S'54-M'57-SM'74-F'77) was born in Helena, MT, on December 10,1928. He received the B.S. degree in 1955, the M.S. degree in 1957, and the Ph.D. degree in 1966, all in electrical engineering, from the University of Washington, Seattle.
From 1947 to 1950 and from 1951 to 1952, he served in the U.S. Air Force as an Electronic's Technician. Between 1957 and 1964, he was a Research Engineer in the Antenna Research Group, Boeing Aerospace Company, Seattle.
While there, his field included research on broad-band and microwave devices, surface-wave antennas, propagation through anisotropic dielectrics, and antennas buried in lossy media. Between 1964 and 1966, he was employed by the Department of Electrical Engineering, University of Washington, conducting research on VLF antennas buried in polar ice caps. At that time, he also served as Consultant to the Department of Rehabilitation Medicine, working on problems associated with the effect of electromagnetic fields on living tissue. In 1966, he joined the faculty of the Department of Rehabilitation Medicine. Presently, he is a Professor in the Center for Bioengineering, has a joint appointment as Professor in Rehabilitation Medicine and adjunct Professor in Electrical Engineering.
Dr. Guy is involved in teaching and research in the area of biological effects and medical applications of electromagnetic energy. He is a member of COMAR, ANSI C-95 Committee, and chairman of
the 1970-1982 Subcommittee IV that developed the protection guides for human exposures to radio frequency fields in 1974 and 1982, NCRP, and chairman of Scientific Committee 53 responsible for biological effects and exposure criteria for radio frequency fields, Armed Forces National Research Council Committee on Vison Working Group 35, Commission A Radio Measurement Methods and URSI, ERMAC, and the EPA Scientific Advisory Board Subcommittee on Biological Effects of Radio
frequency Fields. Dr. Guy also serves as a consultant to the NIEHS on the USSR-US Environmental Health Cooperative Program, and was a member of the NIH Diagnostic Radiology Study Section 1979-1983. Dr. Guy is a member of the editorial boards of the Journal of Microwave Power and IEEE TRANSACTIONS ON MICROWAVE THEORY AND TECHNIQUES, and is current president of the Bioelectromagnetics Society. Dr. Guy holds memberships in Phi Beta Kappa, Tau Beta Pi, and Sigma XI. He is also a member of the American Association for the Advancement of Science.
DARSONVAL.jpg
DARSONVAL_Fig2.jpg
DARSONVAL_Fig3.jpg
DARSONVAL_Fig4.jpg
{kind=link}
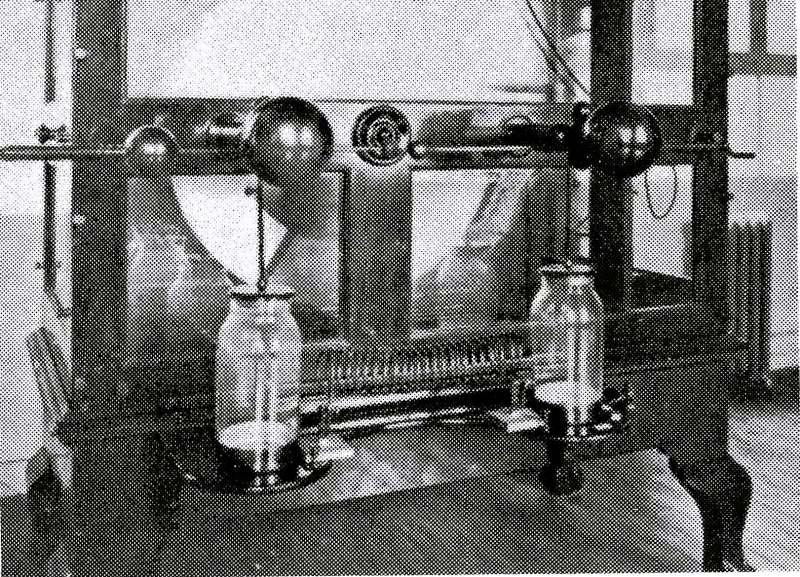{kind=link}
{kind=link}
{kind=link}